What is ‘Blended Care’ and How Does it Work?
 Too busy to drive to the therapist? Looking for a cost-effective way to treat anxiety, depression, or…hoarding disorder?
Too busy to drive to the therapist? Looking for a cost-effective way to treat anxiety, depression, or…hoarding disorder?
Blended care is one potential option for people who have limited access to conventional face-to-face counseling, offering lower costs, less time commitment, and greater flexibility for the patient. So what is blended care exactly, and how does it work?
Before you continue, we thought you might like to download our three Positive Psychology Exercises for free. These science-based exercises will explore fundamental aspects of positive psychology including strengths, values, and self-compassion, and will give you the tools to enhance the wellbeing of your clients, students, or employees.
This Article Contains:
- What is Blended Care?
- How Does It Work?
- Self-Paced Activities in Blended Care (Incl. Quenza)
- Practical Benefits of Blended Care
- Blended Care vs. eHealth
- Is It For Me? The Fit For Blended Care Instrument
- A Look at the Research
- Are There Disadvantages to Blended Interventions?
- A Take-Home Message
- References
What is Blended Care? A Definition
In psychology, blended care refers to a mixture of online therapy (e-therapy), and in-person treatment for a range of disorders. Its underpinning logic is that psychological treatment can be made more accessible by delivering at least part of an intervention online, to help improve patients’ mental health.
A Definition of Blended Therapy
Blended care, which can involve internet-based cognitive behavioral therapy (iCBT) or psychotherapy, involves the collaboration of a therapist who typically provides some support and guidance to the person seeking treatment. It has effectively been used – studies show – to help people manage mental health conditions such as depression and anxiety while improving their coping skills, affect, and wellbeing (Massoudi et al., 2017).
Research suggests that when delivered correctly, blended care can be a promising way to treat anxiety and mood disorders without the need to visit a therapist in person each week. Wentzel and colleagues (2016: 2) describe it succinctly as:
“treatments…in which a combination of online (or mobile) components and face-to-face components is applied.”
Elsewhere in the literature, Massoudi et al. (2017: 2) define blended care in BMC Psychiatry as: “web-based interventions guided by a therapist.”
So, how does it work? If the idea of online counseling to improve your mental health sounds confusing, it’s worth taking a closer look.
How Does it Work?
One of the main challenges with blended care is that no “fixed formula” exists for how it should look (Wentzel et al., 2016). As such blended therapy can draw on a range of different technologies and entail different levels of involvement from the therapist at varying times using a combination of discussion, self-lead activities, and guided exercises.
The balance between these different components is primarily determined based on discussion and subsequent agreement between the therapist and client. Nonetheless, the aims of the therapy pursued via blended care remain largely the same as those pursued through traditional therapy.
For instance, a therapist and client might work through a pre-designed treatment plan, such as an Acceptance and Commitment Therapy (ACT) course or Mindfulness-based Stress Reduction (MBSR) program with the aim to reduce the impact of negative emotions in the client’s life (Andrews, Cuijpers, Craske, McEvoy & Titov, 2010; Fitzpatrick, Nedeljkovic, Abbott, Kyrios & Moulding, 2018; Spek et al., 2007).
This overarching aim may be achieved using one or more approaches that make up blended care. For instance, some blended care practitioners may supplement in-person therapy sessions with another means of digital communication, such as that via phone, videoconferencing, or SMS.
Alternatively, the therapist may assign activities such as reflections, guided meditations, or assessments to complete in between real-time/in-person sessions.
Let’s explore the latter a little closer with an example.
Self-Paced Activities in Blended Care (Incl. Quenza)
As a therapist, it is important to make the most of your limited real-time interactions with your client in the ‘chair.’ This is just one reason why you might encourage your clients to complete more time-consuming activities or exercises outside the therapy room in a self-paced fashion.
A blended care approach that incorporates digital technology can facilitate the design, sharing, and completion of this self-paced work. To illustrate, let’s consider the fictional example of Michael, who is undergoing MBSR therapy to help gain control of his anger and reduce stress.
The therapist wishes to use the principles of MBSR in combination with traditional CBT frameworks to help Michael understand how his interpretation of events and inattention to sensations in his body may be unnecessarily feeding into his experience of stress and angry outbursts.
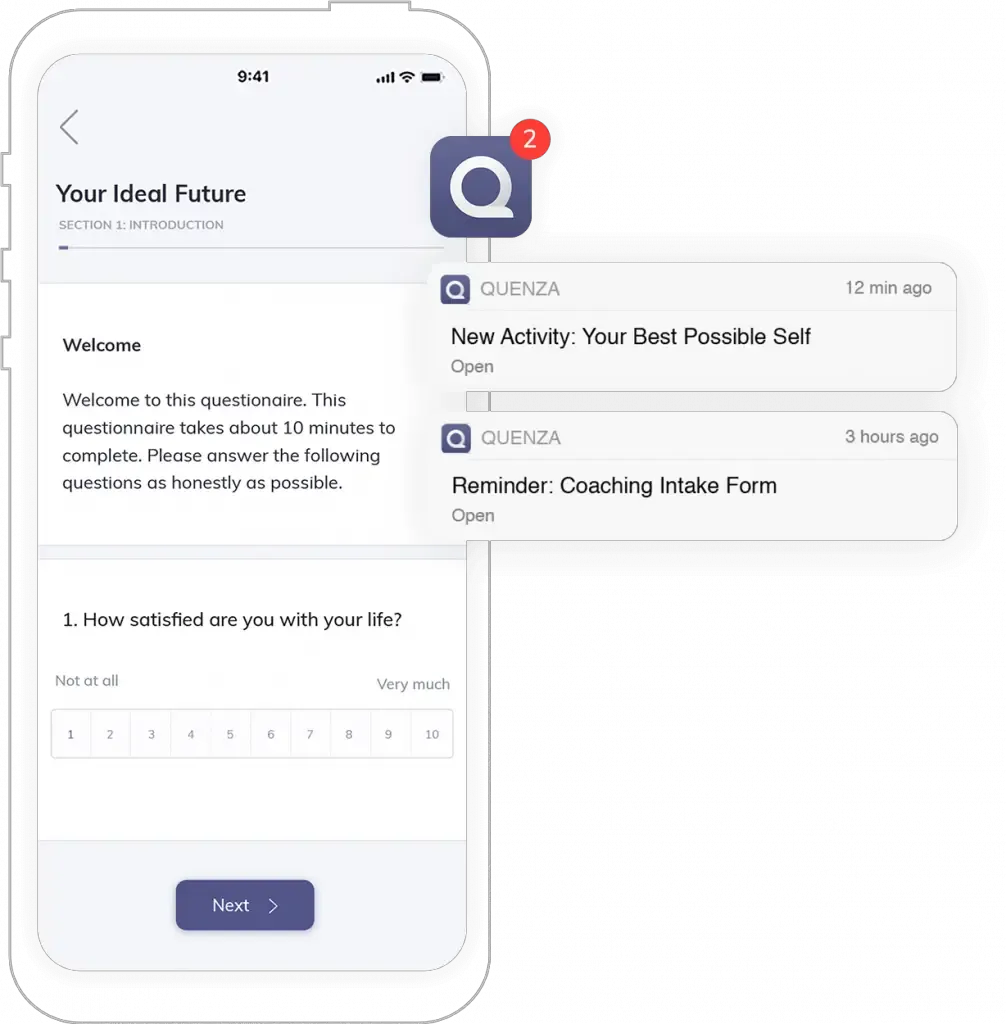
To support the therapist in helping Michael achieve his therapy aims, a blended care approach is used by assigning Michael a customized pathway of self-paced activities, designed and delivered through the platform Quenza (pictured here).

After their first in-person session, the therapist sends Michael his first activity — a standardized assessment of anger. This questionnaire is sent to Michael’s Quenza account to complete at his convenience via his smartphone or tablet, and the therapist will receive the results instantly upon the survey’s completion.
Once Michael completes the assessment, he is automatically sent the next activity in the pathway — a short questionnaire assessing his experience of stress.
A few days after completing this second questionnaire, Michael is automatically sent his third activity — a video lesson exploring how negative emotions manifest as patterns of energy in the body, which can be eased through mindful attention. This is then followed up with a guided audio meditation to help Michael begin to practice these mindfulness principles.
As you can see, using Quenza to facilitate a blended care approach, the therapist has completed much of the initial legwork in Michael’s treatment. The therapist now has the results of his initial anger and stress assessments, which can be reflected on between now and Michael’s second session.
Michael has also been provided resources to give him the initial confidence that his anger and stress can be managed, while also providing him a practice meditation to get started.
This is just an example of how you might integrate a blended care approach into your counseling practice using a platform like Quenza. If you’d like to learn more about Quenza as a tool for providing customized blended care, take a look at our Quenza Interventions article.
Practical Benefits of Blended Care
 There are a range of benefits for clients undergoing blended care interventions (Fitzpatrick et al., 2018):
There are a range of benefits for clients undergoing blended care interventions (Fitzpatrick et al., 2018):
- The client pays for fewer in-person counseling sessions;
- They can access the internet-based content at a time that’s convenient to them;
- They can take a more active role in the process and see it through (due to this greater convenience); and
- The client can receive treatment which their condition(s) might otherwise prohibit them from seeking – e.g., for patients with social anxiety or agoraphobia.
Advantages to practitioners can include greater engagement on the part of their patient, and reduced time commitments on their side.
With fewer face-to-face interactions throughout the treatment, practitioners can potentially also decrease the waiting time between direct interactions and online follow-up support.
Self-paced activities, such as the above example, can also keep clients engaged between sessions. Likewise, the client’s experience of any self-paced activities may serve as a useful focus for discussion during their next in-person session with the therapist.
Through collaboration, patients and their professionals can identify an ideal combination of in-person and online treatments for their therapeutic goals.
When it becomes apparent that a blended care approach will suit both parties, therapists can take advantage of emerging blended care technologies, such as Quenza, to streamline elements of the therapy that can be digitized and help clients achieve their goals through modes that are most convenient for them.
Blended Care vs. EHealth
So what is eHealth, and is it the same as blended care? The short answer is no.
Strictly speaking, the term ‘eHealth’ implies e-therapy, or the ‘internet-only’ side of things, as the UK’s National Health Service explains (DigitalHealth.net, 2019). Due to shrinking workforces and rising demand for mental health support, healthcare providers in countries such as the UK have begun to look increasingly more into online treatment options.
The immediate goal of eHealth is to increase the likelihood of patients receiving timely, good-quality healthcare that can improve their quality of life. But more importantly, as medical providers and government bodies are quick to advise, the ultimate goal is to free up professional time in the long run for blended treatment, which utilizes both face-to-face therapy and eHealth (Andrews et al., 2010).
In other words:
- In-person sessions can deliver high-quality treatment, while eHealth is viewed as a time-saving complement for dealing with lower-level issues; and
- Blended care can save a patient considerable travel costs while still keeping critical face-to-face sessions as part of their treatment.
Curious about whether blended care might suit you or your client? Let’s look at what both therapists and patients will need to consider.

Download 3 Free Positive Psychology Exercises (PDF)
Enhance wellbeing with these free, science-based exercises that draw on the latest insights from positive psychology.
Is It For Me? The Fit For Blended Care Instrument
For blended care to work, there needs to be a fit between the patient’s requirements and the treatment provided. But what does that mean exactly, and how can a mental health practitioner design a blended intervention that meets the needs, abilities, and desires of a patient?
Wentzel and colleagues’ (2016) research suggests that proper communication is the answer. In fact, they’ve created a “Fit For Blended Care Instrument” that helps practitioners shape a dialogue with their patients and elicit the solutions needed to design an appropriate blended treatment.
Making The Most of Blended Therapy
According to the authors, the practical application involves five things:
- Online and face-to-face elements of therapy must be related to one another, not two separate strands of treatment;
- Offline and online components must both contribute in the same way to a patient’s therapy;
- The amount of online and in-person therapy should be tailored to meet the client’s specific needs, not arbitrarily decided (e.g., 50/50);
- Online aspects of the treatment should be flexible and dynamic to engage the patient and remain relevant to the intervention as a whole; and
- Practitioners should consider the patient’s fit with online technology and decide why and how different eHealth or in-person treatments should be used.
Putting these together, then, the Fit For Blended Care Instrument offers questions and a checklist that mental health professionals can use to assess the appropriateness of blended therapy and design an intervention that works.
For instance, (Wentzel et al., 2016):
- Do suitable internet-based modules exist that are linked to the client’s key symptoms?
- Are they experiencing an immediate crisis, such as psychotic symptoms or suicidality?
- Can they access a secure, private place to do online therapy?
- Are their written skills adequate for a blended intervention?
- Are there other potential reasons they might be a good candidate for blended therapy – e.g., not wanting to leave the house, embarrassed to come to the surgery, no time off work?
- Do they have a social support network they can rely on?
By looking at prerequisites for blended treatment, potential obstacles, potential facilitators, and summarizing it as an overview, therapists can make more informed decisions about how to make the most of the treatment’s possibilities.
A Look at the Research
So, when might someone seek out blended care? According to the research, blended therapy has proven itself effective in helping reduce the symptoms of common health conditions, such as mood disorders and anxiety.
Mood Disorders
One 2013 study by Månsson and colleagues, for example, examined a relatively small sample of 15 participants with mild-moderate depression, anxiety, or both. They underwent a 9-week blended care model that involved face-to-face CBT with a therapist and a host of internet-accessible iCBT manuals to complement it, then assessed the patients’ symptoms both immediately afterward and 12 months later.
While this study did not involve a control group, the patients’ symptom scores had decreased by the end of the blended intervention and remained reduced at the 1-year mark – none dropped out, and overall, it has described the blended care model as a helpful support system.
Hoarding Disorder
Another study has revealed similar behavioral improvements for hoarding disorder (HoPE) sufferers whose intervention was a blend of group therapy and iCBT. Fitzpatrick and colleagues’ (2016) e-therapy component included modules on motivation, relapse prevention, goal-setting, and psychoeducation that participants completed over eight weeks.
At the end of the program, participants who underwent blended care had significantly less clutter in their environments – one metric used to assess hoarding severity – than waitlisted participants who received no treatment. A complicated psychological disorder, some findings of blended therapy’s efficacy are a promising step for HoPE sufferers, who make up 2-5 percent of the population.
Substance Abuse
Blended interventions have also shown their efficacy in the treatment of people struggling with substance misuse (Erbe et al., 2017). Not only are they a feasible method of treatment for those with drug and alcohol dependencies, but they were also reasonably cost-effective for both patients and the clinic and had a positive impact on substance use in the long run (Carroll et al., 2009; Olmstead et al., 2010).
Are There Disadvantages to Blended Interventions?
Of course, blended therapy is not for everyone – as the Fit For Blended Care Instrument shows, there are practical issues involved when a large part of the treatment takes place online.
If you’re thinking about blended therapy, some issues to be aware of include (Wentzel et al., 2016):
- Ensuring appropriate digital materials are used, that patients can use them productively, and that they are an optimal complement for the face-to-face element of a psychological intervention;
- Making sure that a blended intervention is a suitable treatment – that a client would not be better off with emergency treatment, for instance;
- That they can access and benefit from the materials as and when they need them, to encourage ongoing use of the content; and
- A therapist must make an informed decision about whether the client can open up in online communications to establish a working relationship.
Last but not least, blended care is intended essentially to be a personalized treatment – what works for one person (or even condition) won’t necessarily be as effective for another. But by supporting face-to-face therapy with online treatment, it offers great potential for patients who want to save money, time, and are happy working through at least some of the process on their own.
A Take-Home Message
Curious about blended therapy? In a day and age of ubiquitous internet, the idea of hopping online to get treatment is compelling.
Blended care offers a cost-effective, time-efficient approach to seeking help when face-to-face sessions with a therapist aren’t practical. For whatever reason – a reluctance to leave the house, or a remote geographical location – online complements to regular interventions can be an effective way of handling difficulties proactively.
Some research suggests that blended therapy may even be easier to stick with, for this reason, potentially helping patients see their treatment through to the end and keep up their wellbeing over time. What are your thoughts on blended therapy, and have you tried it before? Share your thoughts in the comments!
We hope you enjoyed reading this article. Don’t forget to download our three Positive Psychology Exercises for free.
- Andrews, G., Cuijpers, P., Craske, M. G., McEvoy, P., & Titov, N. (2010). Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: a meta-analysis. PloS one, 5(10), e13196.
- Carroll, K. M., Ball, S. A., Martino, S., Nich, C., Babuscio, T. A., & Rounsaville, B. J. (2009). Enduring effects of a computer-assisted training program for cognitive behavioral therapy: a 6-month follow-up of CBT4CBT. Drug and alcohol dependence, 100(1-2), 178-181.
- DigitalHealth.net. (2019). Blended care: a remedy for mental health provision. Retrieved from https://www.digitalhealth.net/2018/07/blended-care-a-remedy-for-mental-health-provision/
- Erbe, D., Eichert, H. C., Riper, H., & Ebert, D. D. (2017). Blending face-to-face and internet-based interventions for the treatment of mental disorders in adults: a systematic review. Journal of medical Internet research, 19(9), e306.
- Fitzpatrick, M., Nedeljkovic, M., Abbott, J. A., Kyrios, M., & Moulding, R. (2018). “Blended” therapy: The development and pilot evaluation of an internet-facilitated cognitive-behavioral intervention to supplement face-to-face therapy for hoarding disorder. Internet interventions, 12, 16-25.
- Månsson, K. N., Ruiz, E. S., Gervind, E., Dahlin, M., & Andersson, G. (2013). Development and initial evaluation of an Internet-based support system for face-to-face cognitive behavior therapy: a proof of concept study. Journal of Medical Internet Research, 15(12), e280.
- Massoudi, B., Blanker, M. H., van Valen, E., Wouters, H., Bockting, C. L., & Burger, H. (2017). Blended care vs. usual care in the treatment of depressive symptoms and disorders in general practice [BLENDING]: study protocol of a non-inferiority randomized trial. BMC psychiatry, 17(1), 218.
- Olmstead, T. A., Ostrow, C. D., & Carroll, K. M. (2010). Cost-effectiveness of computer-assisted training in cognitive-behavioral therapy as an adjunct to standard care for addiction. Drug and alcohol dependence, 110(3), 200-207.
- Richards, D., & Richardson, T. (2012). Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clinical Psychology Review, 32(4), 329-342.
- Spek, V., Cuijpers, P. I. M., Nyklíček, I., Riper, H., Keyzer, J., & Pop, V. (2007). Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: a meta-analysis. Psychological medicine, 37(3), 319-328.
- Van Ballegooijen, W., Cuijpers, P., Van Straten, A., Karyotaki, E., Andersson, G., Smit, J. H., & Riper, H. (2014). Adherence to Internet-based and face-to-face cognitive behavioral therapy for depression: a meta-analysis. PloS one, 9(7), e100674.
- Wentzel, J., van der Vaart, R., Bohlmeijer, E. T., & van Gemert-Pijnen, J. E. (2016). Mixing online and face-to-face therapy: how to benefit from blended care in mental health care. JMIR mental health, 3(1), e9.
Let us know your thoughts
Related articles



Read other articles by their category
- Body & Brain (42)
- Coaching & Application (54)
- Compassion (26)
- Counseling (50)
- Emotional Intelligence (24)
- Gratitude (18)
- Grief & Bereavement (21)
- Happiness & SWB (40)
- Meaning & Values (25)
- Meditation (20)
- Mindfulness (44)
- Motivation & Goals (43)
- Optimism & Mindset (32)
- Positive CBT (25)
- Positive Communication (20)
- Positive Education (45)
- Positive Emotions (30)
- Positive Leadership (14)
- Positive Psychology (32)
- Positive Workplace (33)
- Productivity (16)
- Relationships (41)
- Resilience & Coping (34)
- Self Awareness (20)
- Self Esteem (36)
- Software & Apps (13)
- Strengths & Virtues (30)
- Stress & Burnout Prevention (34)
- Theory & Books (44)
- Therapy Exercises (35)
- Types of Therapy (58)
What our readers think
Katie, the piece is quite insightful and educating. A great resource for lay mind interested in psychology, particularly, ‘blended care’. Thanks.
Thanks for the kind words! I’m glad you found it interesting 🙂
The information provided about blended care was very useful in helping me to gain a better understanding of how blended therapy can help people who are depressed or anxious. It was also really helpful that both arguments for and against e.g. the pros and cons were openly and honestly discussed.
Very helpful and can see how blended therapy would be beneficial to some of my clients who live remotely.
Thank you.
Dear Catherine, Something new to me. thank you so much for sharing this. As always some people may favour this while others would prefer to see face to face consultation. However, this method is an option, the client can make their choices. Personally, I am happy with this. This method is handy for clients who are unwell to cue to be consulted or no one to baby sit their kids for instance.
Thank you again
So happy that you found it useful. I agree with you; there are many reasons why an online component can be a convenient complement to face-to-face therapy. Your examples give two great scenarios in which I believe blended care could improve the likelihood of patients completing treatment despite obstacles.
Thank you Che Gon.
It’s clear that the powerful power differential would start to be eroded when client and therapist work together in blended therapy for the good of the client. A great chance to really put client’s first.
very true, but there should be a questionnaire for therapists for registration who could help needy. Since the idea is good, this must be circulated widely and and a suggestive questionnaire designed for every patient and therapists should be able to customize the questions. Payments must go to therapists so that interest is kept for them to work and help others.
Blended therapy sounds like a great idea for people that are afraid to leave their houses or for people that work and can’t find a therapist but what about insurance and do they pay for it? Some one like me can not afford to pay out of pocket otherwise I would be doing therapy on my cell.