What is Psychodynamic Therapy? 5 Tools & Techniques
 “How does that make you feel?”
“How does that make you feel?”
This question is probably quite familiar to you.
It is the question most often used in pop culture to indicate or reference therapy. It is also the hallmark of psychodynamic therapy.
Ironically, this phrase that immediately calls to mind the practice of therapy is the signature phrase of a type of therapy that is much less common these days. The most popular types of therapy today are actually cognitive behavioral therapy (CBT), interpersonal therapy (IPT), and other, more modern forms of therapy.
While psychodynamic therapy is still applied in many situations, its popularity has lagged behind these other types of therapy in the last few decades.
However, it is still the most recognizable form to those inexperienced in the theory and application of therapy, and it is still a worthwhile goal to understand the basics of psychodynamic therapy.
In this article, we will learn about the theory behind this seemingly simple question to psychodynamic therapy.
But before you continue, we thought you might like to download our three Positive Psychology Exercises for free. These science-based exercises explore fundamental aspects of positive psychology including strengths, values, and self-compassion, and give you the tools to enhance the wellbeing of your clients, students, or employees.
This Article Contains:
What is Psychodynamic Therapy? A Definition
Psychodynamic therapy is a “global therapy,” or form of therapy with a holistic focus on the perspective of the client. The alternative, “problem-based” therapies, such as cognitive-behavioral therapy, aim to reduce or eliminate symptoms instead of exploring the client’s deep-seated needs, urges, and desires (McLeod, 2014).
This translates into significant differences between these therapies in terms of goals, techniques, and general approach.
“In contrast [to behavioral therapy], dynamic psychotherapy, which facilitates a patient’s rewriting of his life narrative, his picture of himself, his past, present, and future, seems uniquely positioned to address the depth of a individual’s experience.”
Richard F. Summers
The global vs. problem-based therapy dichotomy is not the only factor that sets psychodynamic therapy apart from these other, more common forms of therapy. Psychodynamic therapy involves the interpretation of mental and emotional processes rather than focusing on behavior (Strupp, Butler, & Rosser, 1988).
Psychodynamic therapists attempt to help clients find patterns in their emotions, thoughts, and beliefs in order to gain insight into their current self. These patterns are often found to begin in the client’s childhood since psychodynamic theory holds that early life experiences are extremely influential in the psychological development and functioning of an adult (Matthews & Chu, 1997).
Psychodynamic therapy aims to help the client identify important pieces of the puzzle that makes them who they are and rearrange them in ways that allow the client to form a more functional and positive sense of self:
“We see the central task of psychotherapy as the rewriting of a more complex and useful narrative of the patient’s life and experience.”
Richard F. Summers
Psychodynamic therapy sessions are intense and open-ended, dictated by the client’s free association rather than a set schedule or agenda. They are typically scheduled once a week and last about an hour. While Freud’s psychoanalytic therapy (described in more detail below) demanded a much greater investment of time, current psychodynamic therapy is generally practiced in a less intensive manner (WebMD, 2014).
Modern psychodynamic therapy also substitutes a pair of chairs for the stereotypical couch and usually places the therapist and client face-to-face rather than keeping the therapist hidden from the client’s view.
In these sessions, the therapist will encourage the client to talk freely about whatever is on their (conscious) mind. The thoughts and feelings discussed will be probed for recurring patterns in the client’s unconscious mind.
This form of therapy is commonly used with clients suffering from depression or anxiety diagnoses, and there is some evidence suggesting that psychodynamic therapy may be as effective in treating depression as other forms of therapy (WebMD, 2014).
Goals of Psychodynamic Therapy
The main goals of psychodynamic therapy are to (1) enhance the client’s self-awareness and (2) foster understanding of the client’s thoughts, feelings, and beliefs in relation to their past experiences, especially his or her experiences as a child (Haggerty, 2016).
This is accomplished by the therapist guiding the client through the examination of unresolved conflicts and significant events in the client’s past.
The assumption in psychodynamic therapy is that chronic problems are rooted in the unconscious mind and must be brought to light for catharsis to occur. Thus, the client must have the self-awareness to discover these unconscious patterns of thought and an understanding of how these patterns came to be in order to deal with them.
Psychodynamic Theory, Perspective, and Key Concepts
 To truly understand psychodynamic therapy, you need to go back to its roots. While this type of therapy has changed over the last century, it is still built on the foundations of some of the earliest work in modern psychology.
To truly understand psychodynamic therapy, you need to go back to its roots. While this type of therapy has changed over the last century, it is still built on the foundations of some of the earliest work in modern psychology.
In the late 19th century, Sigmund Freud was working on his grand idea of the human mind and the theory of human development. His theories laid the foundation for decades of psychological research and practice.
While many of these theories were eventually found to conflict with hard evidence gained through scientific research, they formed the basis for psychodynamic theory and sparked a bold new school of thought that still exists today, in a modified and updated form.
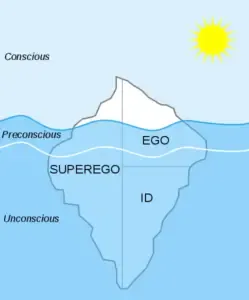
He proposed that the human mind is composed of three parts:
- The id, which consists of instinct and forms the basis of the unconscious mind;
- The superego, or moral component that houses our beliefs of right and wrong;
- The ego, the mediator between the animal instinct of the id and the enlightened moral thought of the superego (Haggerty, 2016).
Freud hypothesized that these components grew out of certain stages in childhood development. He believed humans are born with the id, develop the ego as a toddler, and add the superego around the age of five. Freud’s hypothesis led him to the logical conclusion (based on his theory) that one’s personality is firmly rooted in their childhood experiences.
While Freud believed that each component formed in each human, the development of each component could be significantly influenced by one’s environment and family relationships. These factors could contribute to the development of a healthy sense of self and effective functioning, or they could trigger the development of neuroses and dysfunctional or distressing patterns of thought.
Whether the development led to positive or negative patterns of thoughts and belief, Freud held that that which truly drives human behavior is buried deep within the human mind, in what he termed the unconscious mind.
Freud theorized three levels of the mind:
- The Unconscious:
This level is where our instincts, deeply held beliefs, and many patterns of thought and behavior reside; we are not consciously aware of anything at this level, but Freud believed the contents of the unconscious mind make up the vast majority of who we are, what we want, and how we behave in order to get what we want. - The Subconscious or Preconscious:
This level is between the conscious and unconscious, and can be called up to consciousness with a purposeful effort from the individual; the contents of this level are just below the surface of consciousness. - The Conscious:
This is the level at which we are fully aware; Freud believed this was the level with the least defining content, the level that makes up only a tiny sliver of who we are.
Based on this theory, Freud insisted that to truly address our issues and solve our problems, we must dig deep into the unconscious level. This is where we store our unspoken values, the beliefs we do not even realize we have, and the patterns of thought and behavior developed in our childhood.
While psychodynamic theory has outgrown many of Freud’s simplistic ideas about human nature, many of the assumptions that underlie the psychodynamic approach are reminiscent of Freud’s work:
- The unconscious mind is one of the most powerful drivers of human behavior and emotion;
- No behavior is without cause—all behavior is determined;
- Childhood experiences exert a significant influence on thoughts, emotions, and behavior as an adult;
- Important conflicts during childhood development shape our overall personality as adults (Freud, 1899).
Freud’s theories directly support the methods of psychoanalysis, but also help form the basis of psychodynamic theory and inform the methods and techniques used in today’s psychodynamic therapy.
Psychoanalysis: The Freudian Approach
While psychoanalysis and modern psychodynamic therapy grew from the same source, there are several important differences between the two forms of therapy.
- First, the timeline and duration of psychoanalysis are far more intensive than modern psychodynamic therapy. Psychoanalysis is generally conducted in two to five sessions per week, lasting several years (McLeod, 2014).
- Second, the physical layout of the office or therapy room is significant—in psychoanalysis, the client (or patient, as they are usually called) lies on his or her back on a couch while the therapist sits behind them, out of their line of sight. In modern psychodynamic therapy, it is much more common for therapist and client to face one another, or at least remain in the other’s field of vision.
- Third, the relationship between therapist and client/patient is much more imbalanced than in modern psychodynamic therapies. The position of the therapist and client suggests a significant imbalance of power, with the therapist acting as a distant and detached expert with techniques and knowledge that will not be shared with the client. Meanwhile, the client acts as a troubled supplicant who relies on the therapist for their expertise in teasing out the dysfunctional thoughts and beliefs that plague them (McLeod, 2014).
Some of the psychoanalytical practices have survived or been adapted for modern use, but this uneven relationship between therapist and client generally does not carry over to current psychodynamic therapy. The therapist’s role has been modified over the last century to alter the hierarchy and provide a more equal setting for treatment.
Role of the Psychodynamic Therapist
 Today, the role of the therapist in psychodynamic therapy is to work with the client to discover the bases for their symptoms.
Today, the role of the therapist in psychodynamic therapy is to work with the client to discover the bases for their symptoms.
The therapist plays this role by encouraging the client to talk about the emotions they are feeling and helping the client to identify recurring patterns in their thoughts, emotions, and behaviors.
They can aid the client in finding the significance of these patterns and discovering the effects they exert upon the client.
One of the most important roles of the therapist is to probe the client’s past. Discussion of the client’s childhood and early life experiences will likely take up a large portion of psychodynamic sessions, as this form of therapy assumes these experiences have a significant impact on the client’s current issues.
The therapist observes how the client interacts within the therapeutic relationship and add their own insight into the client’s relationship habits to the discussion.
The psychodynamic theory holds that how the client acts in the relationship with the therapist usually mirrors how they act in other relationships, such as with a parent or other important adult from their childhood (WebMD, 2014).
In general, the therapist’s role is to aid the client in connecting the dots between their past experiences and their current problems, and leverage their internal resources to address these problems.
Introduction to Psychodynamic Theory and Therapy – Perennial Psychology
Types of Psychodynamic Therapy
Throughout this piece, I have referred to psychodynamic therapy as a singular entity to make the discussion of psychodynamic therapies easier; but truthfully writing, psychodynamic therapy is more a category of therapies rather than a single type.
All of the therapies below are grounded in the same overarching model of psychodynamic theory, but they apply the tenets of this theory in different ways.
1. Brief Psychodynamic Therapy
The aspect of brief psychodynamic therapy that sets it apart from other types of psychodynamic therapies is right in the name: brief.
This type of therapy is generally conducted over the course of only a few sessions, or even just one session in some cases. Sometimes an individual struggling with a specific problem only needs to make a few important connections to overcome that problem.
For instance, if a client is suffering from acute anxiety with no known source, the identification of an event or circumstance that gave rise to this anxiety and a strategy for coping can be accomplished in one session.
While the resolution of problems should not be expected in one session for all those seeking treatment, there are several instances where identifying and dealing with a specific problem can be a relatively brief investment.
Brief psychodynamic therapy has been applied to situations like:
- Rape;
- Accident (traffic, physical injury, etc.);
- Act of terrorism;
- Acute psychological disturbances (like anxiety or depression);
- Traumatic family event (discovery of a secret, divorce, etc.).
For more information on brief psychodynamic therapy, visit this link.
2. Psychodynamic Family Therapy
This form of psychodynamic therapy is practiced in the context of a family, whether that family is comprised of two adults in a romantic relationship, a parent and child(ren), siblings, grandparents and grandchildren, a traditional nuclear family, or any combination of these family members.
This therapy is usually relatively long-term (versus the shorter term family therapy based on CBT or IPT) and often is instigated by chronic problems in the family (rather than a significant event or the emersion of a specific problem in the family).
Like other psychodynamic therapies, this form focuses on unconscious processes and unresolved conflicts but views them in the context of family relationships. The therapist will lead the family members through an exploration of family history, especially any traumatic family events.
Often, this form of therapy emphasizes the importance of the adult members of the family working out any conflicts with their own parents as a way to better understand the conflicts with their partner(s) and child(ren).
Psychodynamic family therapy can help families to discover and address the deep-seated issues that give rise to family problems, leading to a healthier and happier family dynamic.
3. Psychodynamic Art / Music Therapy
This non-traditional form of psychodynamic therapy involves the expression of feelings and emotions through art or music.
Like other types of psychodynamic therapy, this therapy is non-directive and non-structured, allowing the client to lead the session. It does not require any artistic or musical talent or ability, only that clients are able to use music or art to express themselves.
Clients may showcase specific pieces and talk about the emotions they evoke, connect them to events from childhood, or discuss the meaning they find in these pieces. Or, clients might bring in a specific song or album that they feel they can relate to on a deep level.
Alternatively, clients can actually create art or music in the session. It doesn’t have to be “good” art or music, it only needs to convey the thoughts or feelings of the clients in a way that makes sense to them.
Through art and/or music, the therapist and client can build an understanding and form an important bond. They may find that art and music are better methods of deep communication than talking.
This type of therapy may be particularly well suited for those who are shy or otherwise find it difficult to talk, as well as clients who are experiencing crippling anxiety or fear which music or art can help to soothe.
You can learn more about psychodynamic music or art therapy through this website or this Prezi slideshow.
5 Psychodynamic Tools and Techniques
 Psychodynamic therapy relies less on exercises and activities than most other types of therapy, but there are some very important tools in the psychodynamic toolbox that allow the therapist to delve deep into the unconscious mind with their clients.
Psychodynamic therapy relies less on exercises and activities than most other types of therapy, but there are some very important tools in the psychodynamic toolbox that allow the therapist to delve deep into the unconscious mind with their clients.
The five tools and techniques below are common practice for many types of psychodynamic therapy.
1. Psychodynamic Diagnostic Manual (PDM)
The Diagnostic and Statistical Manual, or DSM, is often referred to as the clinical psychologist’s Bible. The DSM serves as a framework for understanding and evaluating behavior within a therapeutic context.
Psychodynamic therapists and theorists sometimes critique the DSM’s focus on observable symptoms and omission of more subjective experiences as criteria for diagnosis.
To solve this problem of disagreement over diagnostic criteria, a Psychodynamic Diagnostic Manual (or PDM) was released in 2006 as an alternative or complement to the DSM. Those practicing psychodynamic therapy may find this manual to be more useful in diagnosing and treating their clients than the standard DSM.
2. Rorschach Inkblots
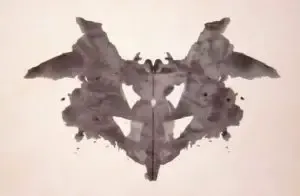 While these ambiguous and untidy splotches of ink are closely connected to Freudian psychoanalysis, they are also used in some forms of psychodynamic therapy today.
While these ambiguous and untidy splotches of ink are closely connected to Freudian psychoanalysis, they are also used in some forms of psychodynamic therapy today.
The Rorschach Inkblot test seems to be a particularly misunderstood tool in the general population.
Pop culture has made the test out to be either an end-all, be-all test of an individual’s personality, unique psychology, and predictor of all manner of mental health maladies, or a useless exercise in naming unnamable shapes.
In fact, the Rorschach test is neither of these things. It cannot illuminate your entire childhood experience, but it is also not a useless bit of trivia from a psychological era gone by.
The original Rorschach inkblots were developed in the early 1900s by psychologist Hermann Rorschach (Framingham, 2016). At the time, a popular game called Blotto involved a set of inkblots that could be organized into a poem or story or used in a round of charades.
Rorschach noticed that patients diagnosed with schizophrenia reacted differently to these inkblots, and began studying their use as a tool for diagnosis and discussion of symptoms.
His work resulted in a set of 10 inkblot images that can be presented to a client with the intention of observing and projecting based on their reactions to the images.
To conduct the Rorschach test, the therapist will present each inkblot to the client individually and ask the client to describe what they see. They are free to use the image as a whole, a piece of the image, or even the blank space surrounding the image to form an interpretation.
The therapist will take notes on the client’s descriptions and how they interpret the image. They may also ask additional questions to get the client to elaborate on what they see.
While there is controversy over how valid and reliable the results of this test should be considered, many therapists find that they provide valuable qualitative information about how the client is feeling and how they think (Cherry, 2017). It has also been found to be somewhat effective in the diagnosis of thinking disorders (such as schizophrenia and bipolar disorder).
Those with these types of disorders tend to see and interpret the images differently than those without such diagnoses.
The important part of this test is the process of interpretation and description undertaken by the client, rather than any specific content seen in the inkblots. As such, the use of this test requires a highly trained professional to conduct, score, and interpret.
To see an online version of this test based on the work of researcher Harrower-Erickson, click here.
3. Freudian Slip
This may be the least formal (and perhaps least applied) technique in psychodynamic therapy, but it is certainly not a dead concept yet.
A “Freudian slip” is also known as a slip of the tongue or, more formally, parapraxes. These slips refer to instances when we mean to say one thing but accidentally let “slip” another, specifically when deeper meaning can be attributed to this slip.
For example, you might call it a Freudian slip when someone intends to say “That is your best idea yet!” but accidentally says “That is your breast idea yet!” You may assume that this individual has a certain anatomical feature in mind, or associates the person they are addressing with said feature.
Another example could be when you are feeling frazzled or overwhelmed at work and your boss pops by for a quick discussion. You aren’t really paying attention, and you absentmindedly say “Thanks Mom” instead of using your boss’ name. A psychoanalyst may consider this slip and decide that you have unresolved issues with your mother and that you are trying to fill the void of that parental relationship with your boss.
Freud (and some subsequent psychodynamic theorists) believed that these “accidental” slips of the tongue are not truly accidental, but actually reveal something meaningful about you. The Freudian theory holds that no behavior is accidental or random; rather, every move you make and every word you say are determined by your mind (conscious, subconscious, or unconscious) and your circumstances.
A psychodynamic therapist may pay special attention to any such slips, whether they occur in session or are simply related by the client during a session, and find meaning in the word substitution. They may conclude that a slip is actually a little piece of your unconscious finding its way to the surface, indicating an unmet desire or unknown association between two concepts.
While most modern psychologists agree that Freudian slips are generally just “slips,” it’s hard to argue that a slip of the tongue can’t occasionally reveal an interesting connection in the speaker’s mind.
4. Free Association
Free association may be the single most important and most used tool for psychodynamic therapists. This technique is simple and often effective.
In the context of psychodynamic therapy, there are two meanings attached to “free association:” the more official therapy technique of free association, and the general method of in-session discussion driven by the client’s free association between topics.
The more formal technique involves the therapist reading a list of words and the client responding immediately with the first word that comes to mind. This exercise can shed light on some of the associations and connections the client has hidden deep below the surface.
This technique may not be as useful to a client who is resistant to the exercise or to sharing intimate details with the therapist. However, therapists should not assume that a client who pauses before responding is resistant—it may indicate that the client is getting closer to a repressed or highly significant connection.
Free association may provoke an especially intense or vivid memory of a traumatic event, called an abreaction. This can be extremely distressing for the client, but it can also lead to a healing experience of catharsis if the client feels like it helped them work through a significant problem (McLeod, 2014).
The less formal concept of free association is simply the tendency to allow the client to lead the discussion in psychodynamic therapy sessions. This kind of relaxed, non-structured approach to dialogue in therapy is a hallmark of psychodynamics.
Practicing this type of informal free association ensures that the therapist is not leading the client anywhere in particular and that the client is moving authentically from one subject to the next. This is critical in psychodynamic therapy, as it is unlikely to reach the unconscious sources of psychological distress without following the client’s lead.
5. Dream Analysis
 Another vestige of Freudian therapy, this highly subjective technique can prove useful for some, although its efficacy as a treatment technique is not proven via the scientific method.
Another vestige of Freudian therapy, this highly subjective technique can prove useful for some, although its efficacy as a treatment technique is not proven via the scientific method.
However, the effectiveness of therapy cannot always be measured and codified by double-blind random control trials (RCTs), the gold standard of research.
Sometimes it is nearly impossible to determine which components or modes of treatment brought about success in therapy.
It is in this ambiguous environment that some of those not-quite-established techniques can contribute to real progress for the client. While dream analysis cannot be formally recommended as a reliable and effective tool, it is unlikely to cause any harm and should, therefore, be left up to the client and therapist whether to include it in the treatment regimen.
Dream analysis is undertaken by discussing the client’s dreams in detail. The therapist will guide the client through this discussion, asking questions and prodding the client to remember and describe the dream in as much detail as possible.
While the client talks about their dream, the therapist will attempt to aid the client in sorting the “manifest” content from “latent” content. The manifest content is what the client remembers about their dream—what happened, who was there, how it felt, the physical and temporal environment of the dream, etc. The latent content is what is beneath the surface of the dream, and this is where the meaning of the dream lies
(McLeod, 2014).
While Freud would nearly always find a repressed sexual urge or sex-related significance in the latent content, today’s dream interpreters have broadened their scope of meaning.
There are nearly countless ways that therapists, coaches, counselors, and practitioners of the more mystical arts engage in dream analysis, none of which have been identified as more effective or useful than the others.
However, one popular method of analyzing dreams comes from psychologist and author Dr. Patrick McNamara. His theory of the dreaming process can be explored on an individual level, allowing the client to attempt to sort through their own dreams to find meaning.
McNamara’s proposed process of dreaming is as follows:
- Step One:
The dreamer disentangles their consciousness from executive control/personal agency. In other words, the dreamer de-identifies with their usual self and sets up a “liminal state”—a state in which the dreamer is prepared to explore a new identity. - Step Two:
The dreamer moves into this liminal space, opening him- or herself up to a world of possibilities in regards to their identity. This step is like taking off your usual “mask” and set it aside in anticipation of finding a new mask. - Step Three:
This step typically occupies the most time and material of the dream, in which the dreamer “tries on” a new identity. The dreamer may be experiencing fear or anxiety associated with shedding their identity, and he or she may seek to reestablish a sense of control by searching for another identity or alternate sense of self. - Step Four:
The dreamer finds a new, altered identity or resumes their old identity. McNamara believes we are searching for a more unified sense of self, but that we often find an identity that includes aspects of our darker side (McNamara, 2017).
These steps are tied into four literary tropes that some believe we use to make sense of the narratives we encounter and experience: metonymy (breaking up the pieces of a narrative), synecdoche (reorganizing those pieces into a new whole), metaphor (comparison of the pieces or the whole with something familiar), and irony (reflection of the new whole).
Using these tools for understanding narrative, McNamara suggests we can apply this process and the literary tropes to parse the meaning of any dream or dream sequence (2017). Of course, this technique has not been proven through scientific research, but you may find it helpful nonetheless.
For more information on McNamara’s system for dream interpretation, click here.
A Take-Home Message
This piece is intended to give you a background in the theory and practice of psychodynamic therapy. This form of therapy paved the way for many of the most popular current forms of therapy and introduced several important ideas to the field of psychology.
While it may not enjoy a place at the top of the therapy hierarchy any longer, it is still a widespread form of therapy that can be effective for many clients, making it a worthwhile topic to explore.
I hope reading this piece has given you a better understanding of the roots of psychodynamic therapy and a more informed idea of what this therapy entails, beyond the clichéd question “How does that make you feel?”
As always, we’d love to hear from you in the comments section! Have you participated in psychodynamic therapy? What was the experience like for you? Did you learn anything significant from your foray into your unconscious mind?
Thanks for reading!
We hope you enjoyed reading this article. Don’t forget to download our three Positive Psychology Exercises for free.
- Cherry, K. (2017). What is the Rorschach inkblot test? Very Well. Retrieved from https://www.verywell.com/what-is-the-rorschach-inkblot-test-2795806
- Framingham, J. (2016). Rorschach inkblot test. Psych Central. Retrieved from https://psychcentral.com/lib/rorschach-inkblot-test/
- Freud, S. (1899). The interpretation of dreams. Vienna, Austria: Franz Deuticke.
- Good Therapy. (2017). Psychodynamic therapy. GoodTherapy. Retrieved from http://www.goodtherapy.org/learn-about-therapy/types/psychodynamic
- Haggerty, J. (2016). Psychodynamic therapy. Psych Central. Retrieved from https://psychcentral.com/lib/psychodynamic-therapy/
- Matthews, J. A., & Chu, J. A. (1997). Psychodynamic therapy for patients with early childhood trauma. In P. S. Appelbaum, L. A. Uyehara, & M. R. Elin (Eds.), Trauma and memory: Clinical and legal controversies (pp. 316–343). Oxford, UK: Oxford University Press.
- McLeod, S. (2014). Psychoanalysis. Simply Psychology. Retrieved from https://www.simplypsychology.org/psychoanalysis.html
- McNamara, P. (2017, March 3). Dream interpretation: How to interpret your dream. Psychology Today. Retrieved from https://www.psychologytoday.com/blog/dream-catcher/201703/dream-interpretation
- Strupp, H. H., Butler, S. F., & Rosser, C. L. (1988). Training in psychodynamic therapy. Journal of Consulting and Clinical Psychology, 56(5), 689-695.
- WebMD. (2014). Psychodynamic therapy for depression. WebMD. Retrieved from http://www.webmd.com/depression/guide/psychodynamic-therapy-for-depression#1
Let us know your thoughts
Related articles


Read other articles by their category
- Body & Brain (42)
- Coaching & Application (54)
- Compassion (26)
- Counseling (50)
- Emotional Intelligence (24)
- Gratitude (18)
- Grief & Bereavement (21)
- Happiness & SWB (39)
- Meaning & Values (25)
- Meditation (20)
- Mindfulness (44)
- Motivation & Goals (43)
- Optimism & Mindset (32)
- Positive CBT (25)
- Positive Communication (20)
- Positive Education (44)
- Positive Emotions (30)
- Positive Leadership (14)
- Positive Psychology (32)
- Positive Workplace (33)
- Productivity (16)
- Relationships (41)
- Resilience & Coping (34)
- Self Awareness (20)
- Self Esteem (36)
- Software & Apps (13)
- Strengths & Virtues (30)
- Stress & Burnout Prevention (34)
- Theory & Books (44)
- Therapy Exercises (35)
- Types of Therapy (58)
What our readers think
There is no one side fits it all kind of intervention. Each case seem to be looked into uniqely
really useful
Very insightful
Thanks a lot for the information. Its very informative and well explained. Kudos to the team and keep it up. God bless you
I tried psychodynamic therapy and have absolutely no clue what was supposed to happen. I asked the one I hired but she was useless. The whole experience was frustrating and useless and I am worse off for having tried it.
Hi, do you have the reference list for this article? very interesting thank you!
Hi Annie,
If you scroll to the very end of the article, you will find a button that you can click to reveal the reference list.
Hope this helps!
– Nicole | Community Manager
Hi there,
Many thanks for describing , with clarity , what is psychodynamic therapy. I have just started sessions with a psychodynamic therapist..only had two sessions so far…but I don’t feel comfortable in the sessions as I sense a lack of empathy and warmth. For example , having established that I had a traumatic childhood and as a result have issues of self-esteem and feelings of ‘not being good enough’ I found it very odd that I was asked certain questions. For example, ‘but your father didn’t care about you, did he? He didn’t care about your education, did he? He only wanted you to work so you could pay for his drink, right? You are very defensive, are you like that with friends? Do you have any friends?
The truth is my father was an alcoholic who had his own issues ( prisoner of war, lost his own father very young) and subsequently was unable to meet my emotional needs. But when he was not drinking he was kind and not a horrid man, if somewhat detached. I have many friends all over the world ,some from 50 years ago! I am popular and make friends easily. So I couldn’t see what the therapist was driving at. Was she trying to make me revisit old wounds? Was this intended to be cathartic? A long time ago I came to terms with my father’s behaviour. I’m a practising Buddhist and as such I see him just living his life , living out his own karma and I just got caught up in the crossfire of his angry struggle with life. As a Buddhist, we also believe that one should never disparage one’s parents. So I found her ( therapist) tone and comments offensive and hurtful.
We have an agreement whereby we give a months notice but I really feel that if I feel so unhappy at this stage, I have to ask myself, what can be accomplished in 3 or 4 more sessions? She will be better off financially but I can’t see how I will be any happier or clearer on emotional issues.
Any advice would be welcome.
With many thanks and best wishes, Jean
‘
Hi Jean,
Psychodynamic is a modern type of psychoanalytic theory. But I will answer to your dilemma with your therapist. I would recommend being honest with your therapist. Share what you felt about those questions, and everything you said here. No one can tell you when to stop the therapy but yes openly sharing your concern will help you make the further decision.
I hope it helps.
Thank you so much for such a great article. I am currently studying a MA in Social Work in the UK. Would you mind posting the Gad, 2017 reference please? I am working on a paper and this would be very helpful. Unfortunately, this reference was not included in the reference list?
Many thanks
Amanda
Thanks for the great article. I’m working on a reaserch paper and would love to quote Gad, 2017. was hoping you could please post it, thanks!
HI did you ever get the GAD reference?
Hi Amanda, Shimon, & Barry,
Our editing team has just taken a look at this, and we believe that citation was a typo. Apologies for the mistake! We have now replaced these with alternative references (you can find full details of the sources in the reference list).
– Nicole | Community Manager
Thanks so much for got my point to stand on
The information was very useful.